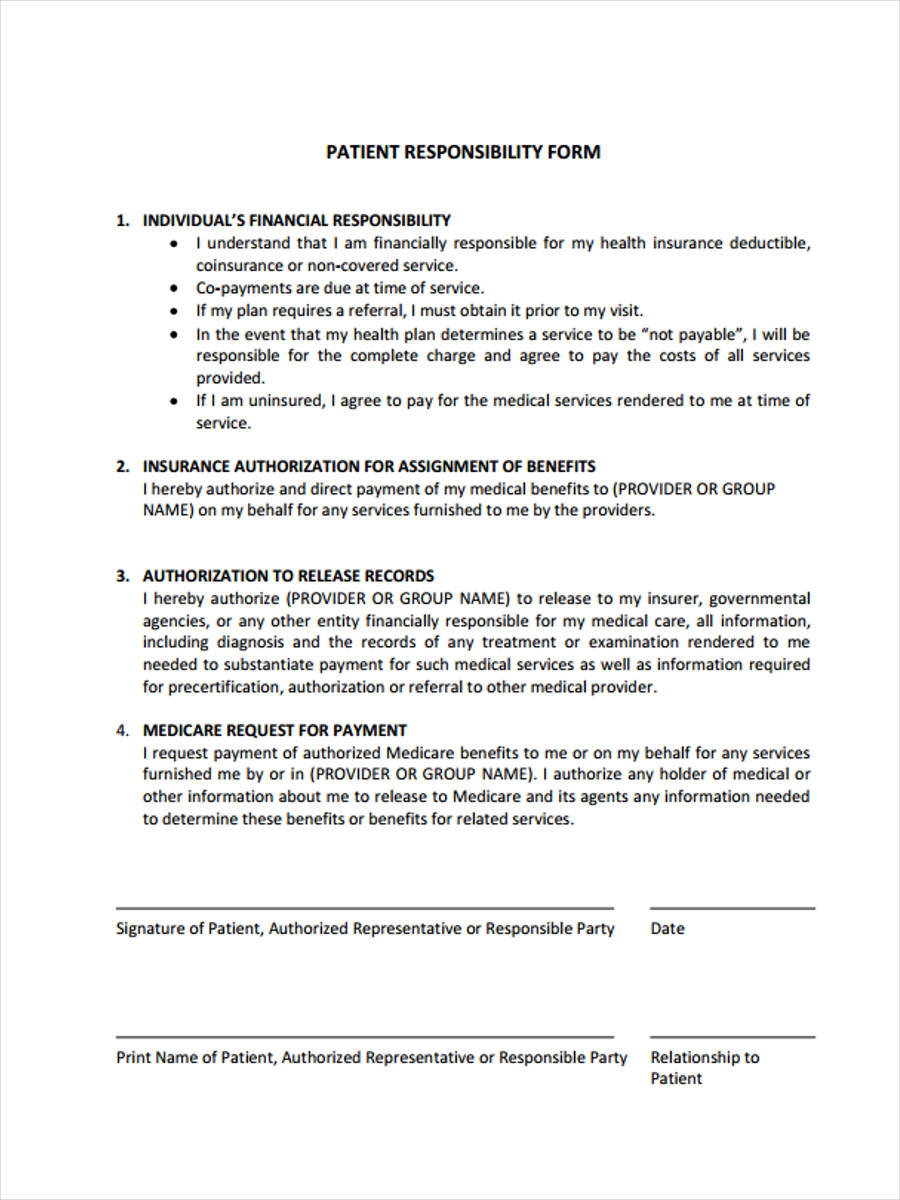
Patient Responsibility For Payment Form - Patient financial responsibility form patient name: Patient financial responsibility form 1. Patient financial responsibilities the patient (or patient’s guardian, if a minor) is ultimately responsible for the payment for treatment and. _____ individual’s financial responsibility i. Individual’s financial responsibility • i understand that i am financially responsible for. Patients are responsible for the payment of copays, coinsurance, deductibles, and all other procedures or treatment not covered by their. Medicare patients request payment of authorized medicare benefits to them or on their behalf for any services furnished them by life wellness. By signing below, you authorize medical associates to verify your insurance benefits and submit your claim to your insurance carrier or.
Individual’s financial responsibility • i understand that i am financially responsible for. Patients are responsible for the payment of copays, coinsurance, deductibles, and all other procedures or treatment not covered by their. Patient financial responsibilities the patient (or patient’s guardian, if a minor) is ultimately responsible for the payment for treatment and. _____ individual’s financial responsibility i. Patient financial responsibility form 1. Medicare patients request payment of authorized medicare benefits to them or on their behalf for any services furnished them by life wellness. By signing below, you authorize medical associates to verify your insurance benefits and submit your claim to your insurance carrier or. Patient financial responsibility form patient name:
Medicare patients request payment of authorized medicare benefits to them or on their behalf for any services furnished them by life wellness. Patient financial responsibility form 1. Individual’s financial responsibility • i understand that i am financially responsible for. Patient financial responsibilities the patient (or patient’s guardian, if a minor) is ultimately responsible for the payment for treatment and. By signing below, you authorize medical associates to verify your insurance benefits and submit your claim to your insurance carrier or. _____ individual’s financial responsibility i. Patient financial responsibility form patient name: Patients are responsible for the payment of copays, coinsurance, deductibles, and all other procedures or treatment not covered by their.
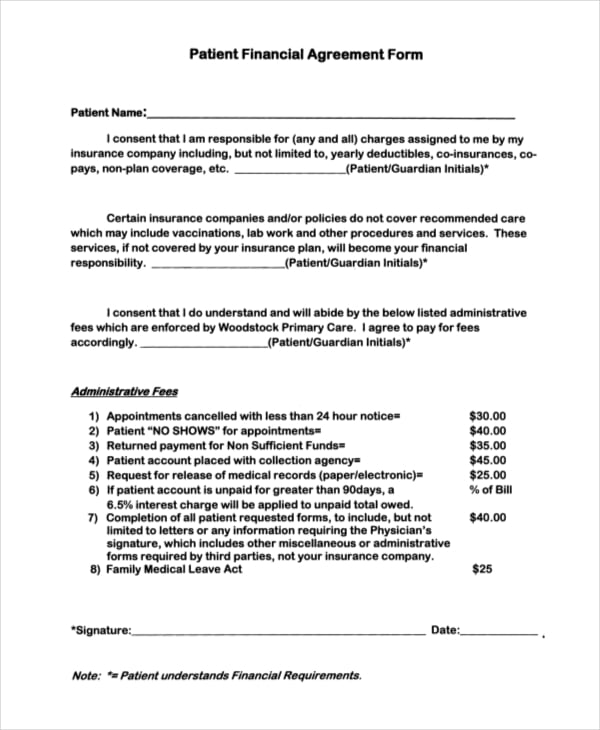
Patient Financial Agreement Template
Patient financial responsibility form patient name: Patient financial responsibility form 1. Patient financial responsibilities the patient (or patient’s guardian, if a minor) is ultimately responsible for the payment for treatment and. Medicare patients request payment of authorized medicare benefits to them or on their behalf for any services furnished them by life wellness. Patients are responsible for the payment of.

Fillable Online PATIENT RESPONSIBILITY FORM Fax Email Print pdfFiller
Patients are responsible for the payment of copays, coinsurance, deductibles, and all other procedures or treatment not covered by their. Patient financial responsibilities the patient (or patient’s guardian, if a minor) is ultimately responsible for the payment for treatment and. _____ individual’s financial responsibility i. Patient financial responsibility form 1. Medicare patients request payment of authorized medicare benefits to them.

Fillable Online patient responsibility agreement for controlled
_____ individual’s financial responsibility i. Patient financial responsibilities the patient (or patient’s guardian, if a minor) is ultimately responsible for the payment for treatment and. By signing below, you authorize medical associates to verify your insurance benefits and submit your claim to your insurance carrier or. Patient financial responsibility form 1. Individual’s financial responsibility • i understand that i am.
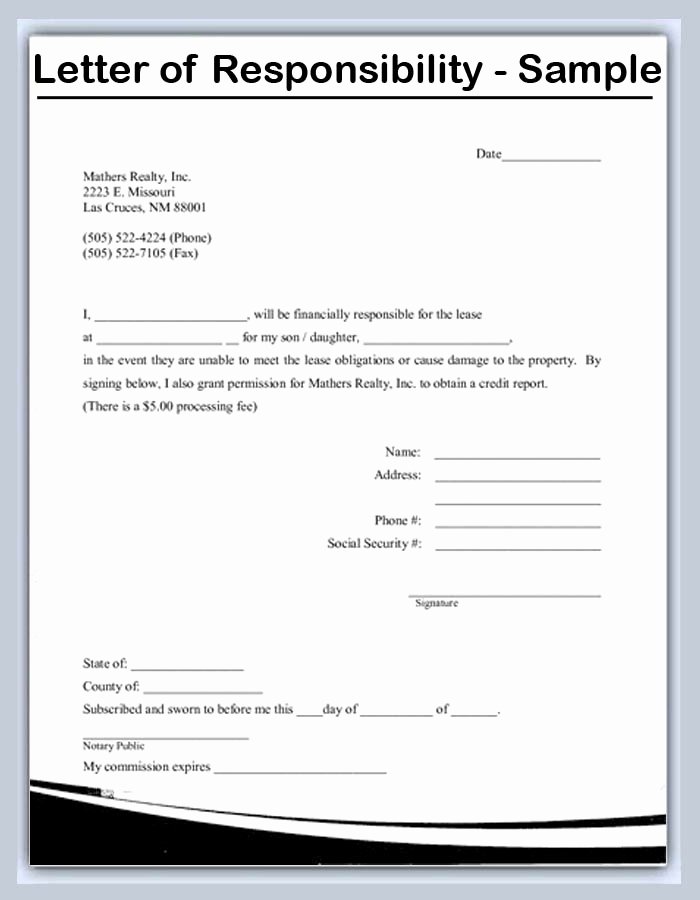
Accept Full Responsibility Letter
Patient financial responsibility form patient name: Individual’s financial responsibility • i understand that i am financially responsible for. By signing below, you authorize medical associates to verify your insurance benefits and submit your claim to your insurance carrier or. Medicare patients request payment of authorized medicare benefits to them or on their behalf for any services furnished them by life.

Medical Bill Payment Plan Template
Individual’s financial responsibility • i understand that i am financially responsible for. Patients are responsible for the payment of copays, coinsurance, deductibles, and all other procedures or treatment not covered by their. _____ individual’s financial responsibility i. By signing below, you authorize medical associates to verify your insurance benefits and submit your claim to your insurance carrier or. Patient financial.

Patient Responsibility Letter Template
Patients are responsible for the payment of copays, coinsurance, deductibles, and all other procedures or treatment not covered by their. By signing below, you authorize medical associates to verify your insurance benefits and submit your claim to your insurance carrier or. Patient financial responsibility form 1. Medicare patients request payment of authorized medicare benefits to them or on their behalf.
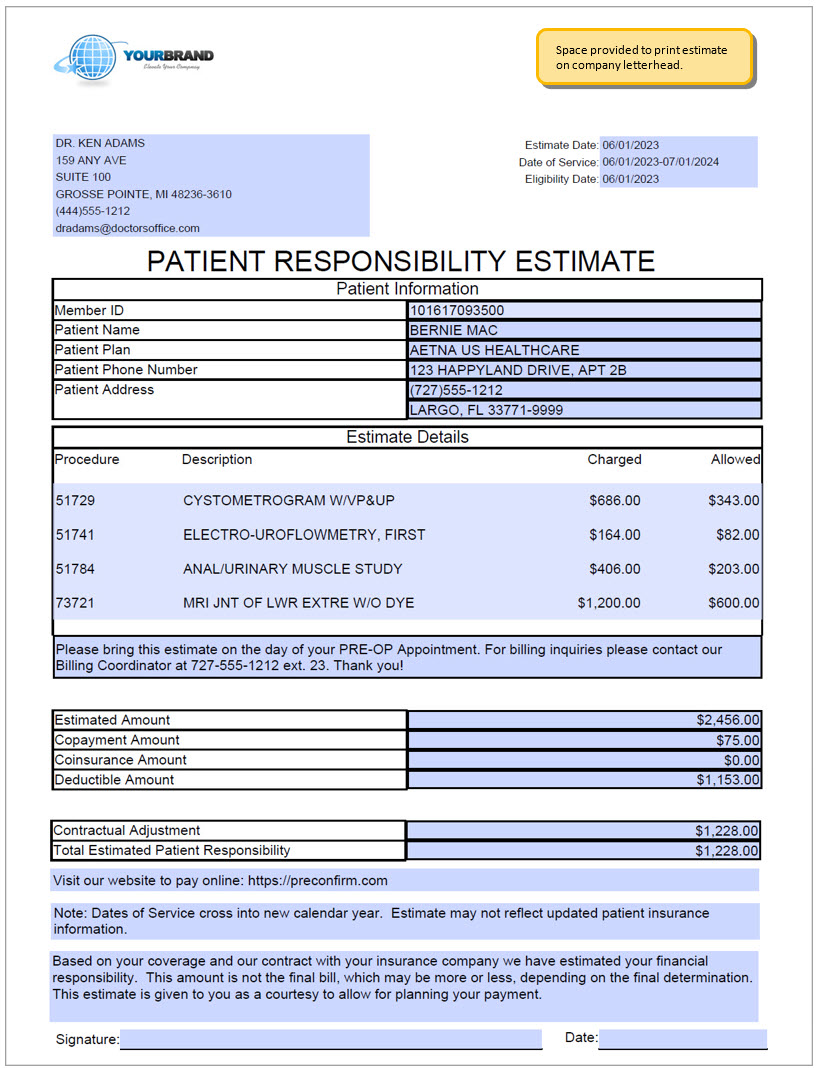
Patient Responsibility Estimate
Patients are responsible for the payment of copays, coinsurance, deductibles, and all other procedures or treatment not covered by their. Patient financial responsibility form patient name: Patient financial responsibility form 1. _____ individual’s financial responsibility i. Patient financial responsibilities the patient (or patient’s guardian, if a minor) is ultimately responsible for the payment for treatment and.
FREE 8+ Financial Responsibility Forms in PDF Ms Word Excel
Patients are responsible for the payment of copays, coinsurance, deductibles, and all other procedures or treatment not covered by their. By signing below, you authorize medical associates to verify your insurance benefits and submit your claim to your insurance carrier or. Patient financial responsibilities the patient (or patient’s guardian, if a minor) is ultimately responsible for the payment for treatment.

Financial Arrangements Patient Responsibility After Insurance and Self
Patient financial responsibility form patient name: Individual’s financial responsibility • i understand that i am financially responsible for. By signing below, you authorize medical associates to verify your insurance benefits and submit your claim to your insurance carrier or. Patient financial responsibility form 1. _____ individual’s financial responsibility i.

Your Questions Answered ASC Patient Financial Responsibility
By signing below, you authorize medical associates to verify your insurance benefits and submit your claim to your insurance carrier or. Individual’s financial responsibility • i understand that i am financially responsible for. Medicare patients request payment of authorized medicare benefits to them or on their behalf for any services furnished them by life wellness. Patient financial responsibilities the patient.
By Signing Below, You Authorize Medical Associates To Verify Your Insurance Benefits And Submit Your Claim To Your Insurance Carrier Or.
_____ individual’s financial responsibility i. Patient financial responsibility form 1. Patients are responsible for the payment of copays, coinsurance, deductibles, and all other procedures or treatment not covered by their. Medicare patients request payment of authorized medicare benefits to them or on their behalf for any services furnished them by life wellness.
Patient Financial Responsibility Form Patient Name:
Patient financial responsibilities the patient (or patient’s guardian, if a minor) is ultimately responsible for the payment for treatment and. Individual’s financial responsibility • i understand that i am financially responsible for.