Ihss Provider Termination Form - Discontinue the provider’s employment with the following recipient: Health and human services agency california department of social. Place the provider in leave. This form will serve as written request to:
Discontinue the provider’s employment with the following recipient: Health and human services agency california department of social. Place the provider in leave. This form will serve as written request to:
Place the provider in leave. Discontinue the provider’s employment with the following recipient: This form will serve as written request to: Health and human services agency california department of social.
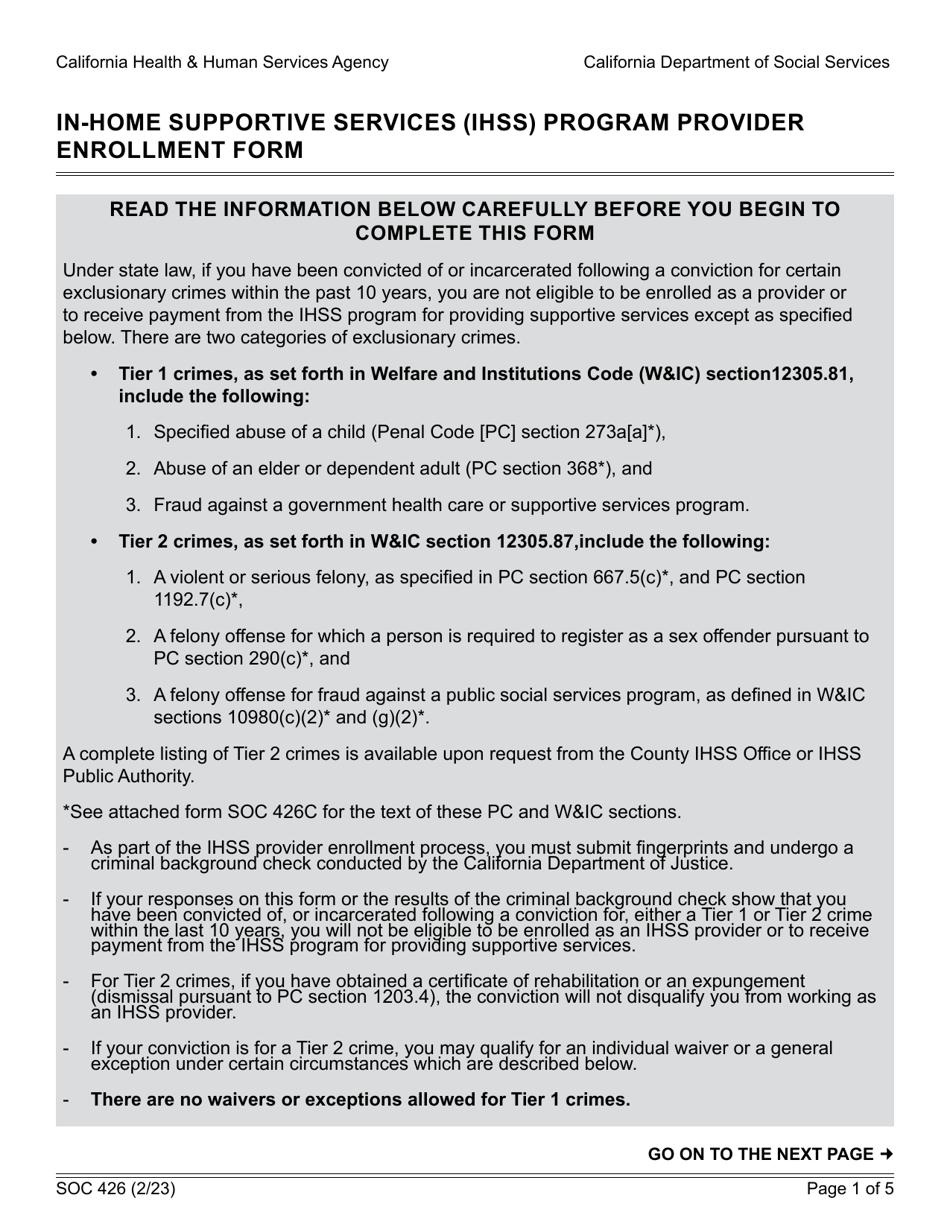
Form SOC426 Download Fillable PDF or Fill Online Inhome Supportive
This form will serve as written request to: Health and human services agency california department of social. Place the provider in leave. Discontinue the provider’s employment with the following recipient:
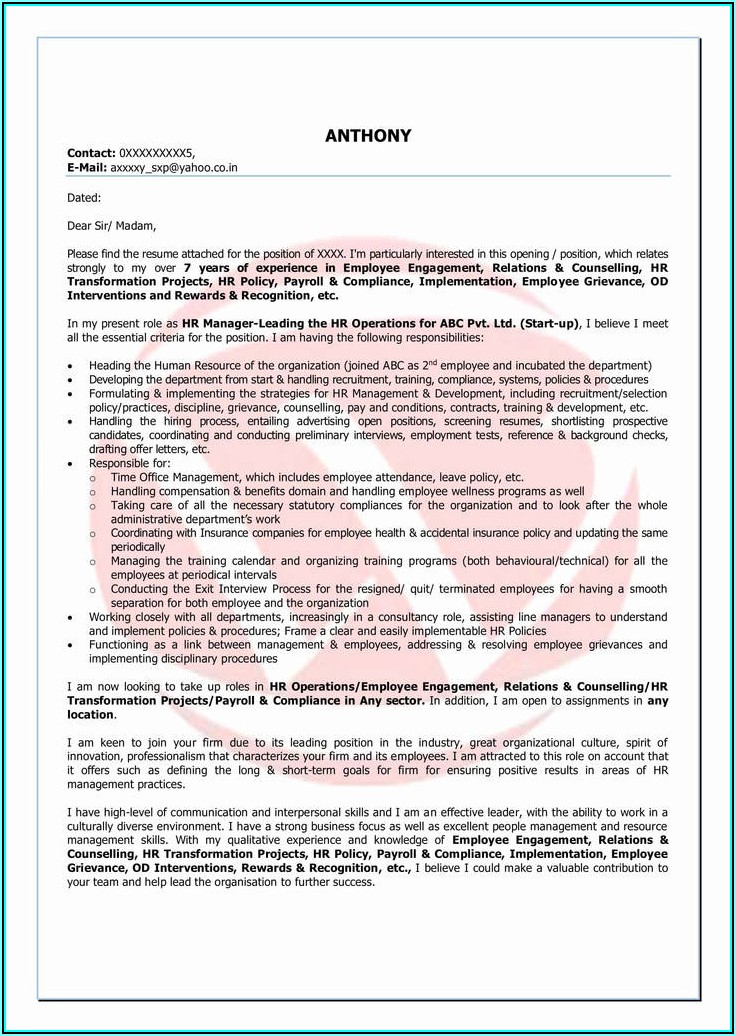
Ihss Provider Enrollment Form Soc 426 Form Resume Examples Wk9yjW0Y3D
Place the provider in leave. This form will serve as written request to: Discontinue the provider’s employment with the following recipient: Health and human services agency california department of social.

Form Soc 2274 InHome Supportive Services (Ihss ) Program
This form will serve as written request to: Health and human services agency california department of social. Place the provider in leave. Discontinue the provider’s employment with the following recipient:
Ihss termination form
Health and human services agency california department of social. Place the provider in leave. Discontinue the provider’s employment with the following recipient: This form will serve as written request to:

Ihss Provider Insurance Application Financial Report
Health and human services agency california department of social. Place the provider in leave. This form will serve as written request to: Discontinue the provider’s employment with the following recipient:
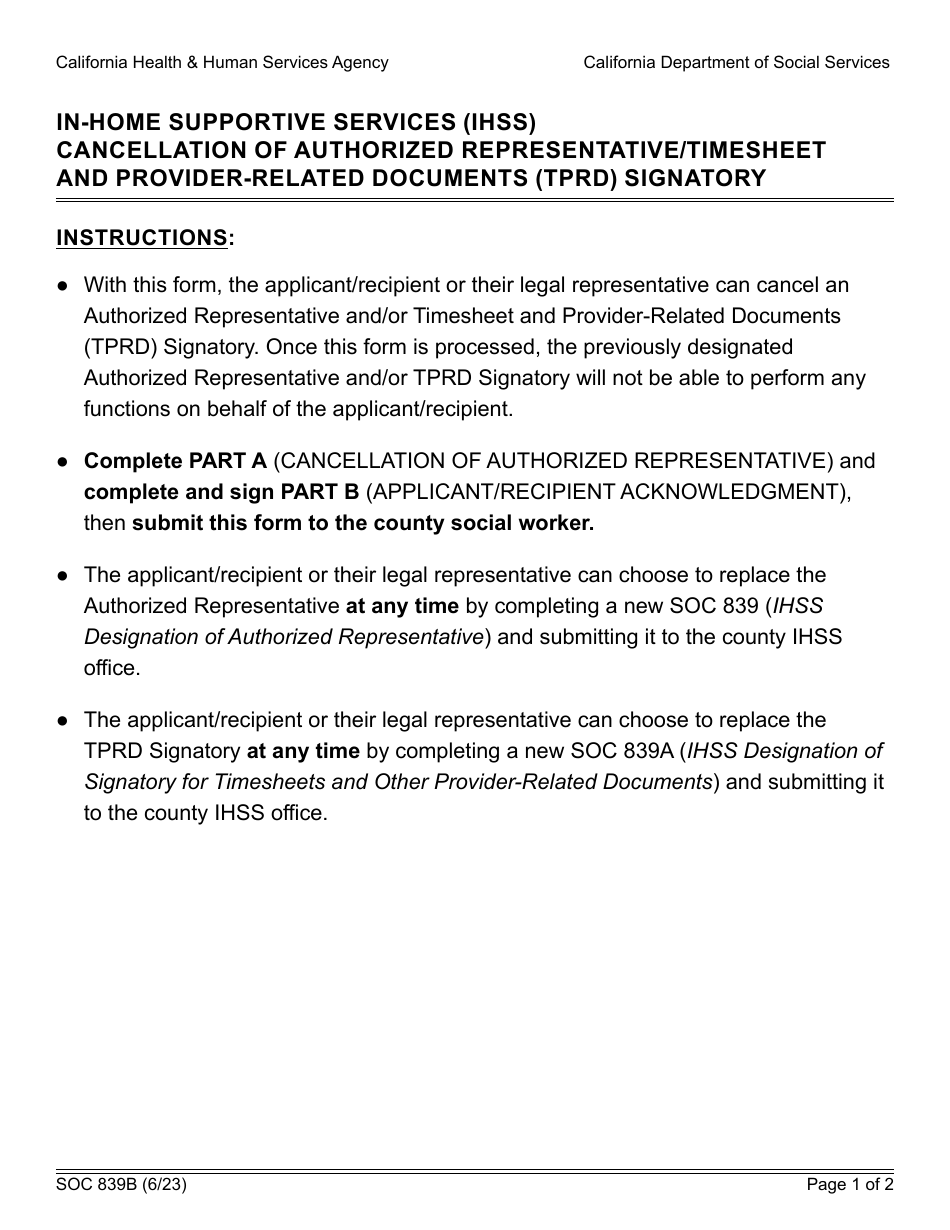
Form SOC839B Fill Out, Sign Online and Download Fillable PDF
This form will serve as written request to: Place the provider in leave. Discontinue the provider’s employment with the following recipient: Health and human services agency california department of social.
Form SOC2312A Download Fillable PDF or Fill Online Inhome Supportive
Place the provider in leave. Health and human services agency california department of social. Discontinue the provider’s employment with the following recipient: This form will serve as written request to:
Ihss termination form
This form will serve as written request to: Place the provider in leave. Health and human services agency california department of social. Discontinue the provider’s employment with the following recipient:
In Home Supportive Services IHSS Program Medical Certification Form
Place the provider in leave. Health and human services agency california department of social. Discontinue the provider’s employment with the following recipient: This form will serve as written request to:
In Home Supportive Services PDF Complete with ease airSlate SignNow
Place the provider in leave. This form will serve as written request to: Health and human services agency california department of social. Discontinue the provider’s employment with the following recipient:
Discontinue The Provider’s Employment With The Following Recipient:
This form will serve as written request to: Place the provider in leave. Health and human services agency california department of social.