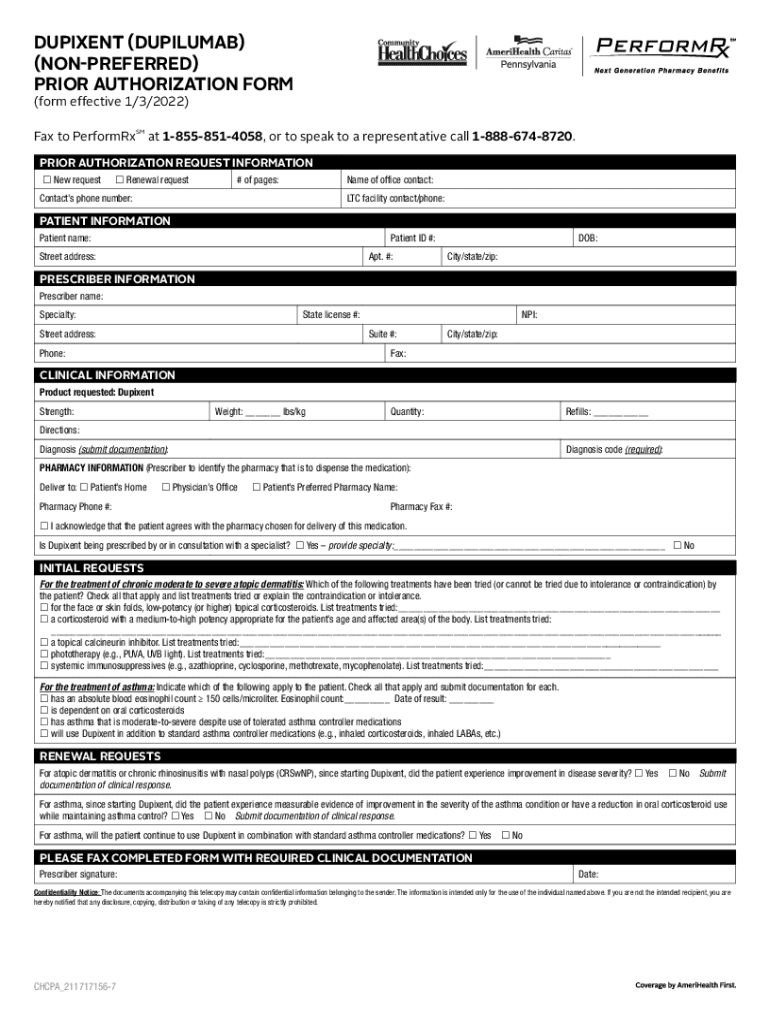
Dupixent Prior Authorization Form - Reduction in the frequency of exacerbations. Obtain the appropriate pa form after initiating your patient through one of the following: Dupixent (dupilumab) (preferred) prior authorization form (form effective 1/8/2024) fax to performrx. Submit a separate form for each medication. • dupixent myway ® • covermymeds • insurance provider •. • dupixent myway® • covermymeds • insurance provider •. Please print, type or write legibly in blue or black. Obtain the appropriate pa form after initiating your patient through one of the following: Please see additional important safety information on next page and accompanying full prescribing information. Authorization will be issued for 12 months.
Authorization will be issued for 12 months. Obtain the appropriate pa form after initiating your patient through one of the following: Prescribed by one of the following: Submit a separate form for each medication. • dupixent myway® • covermymeds • insurance provider •. Obtain the appropriate pa form after initiating your patient through one of the following: Please see additional important safety information on next page and accompanying full prescribing information. Instructions for completing this form 1. Reduction in the frequency of exacerbations. • dupixent myway ® • covermymeds • insurance provider •.
• dupixent myway® • covermymeds • insurance provider •. Authorization will be issued for 12 months. Prescribed by one of the following: Dupixent (dupilumab) (preferred) prior authorization form (form effective 1/8/2024) fax to performrx. Please print, type or write legibly in blue or black. • dupixent myway ® • covermymeds • insurance provider •. Obtain the appropriate pa form after initiating your patient through one of the following: Please see additional important safety information on next page and accompanying full prescribing information. Obtain the appropriate pa form after initiating your patient through one of the following: Instructions for completing this form 1.
Fillable Online Dupixent Prior Authorization Form Pharmacy
Dupixent (dupilumab) (preferred) prior authorization form (form effective 1/8/2024) fax to performrx. Instructions for completing this form 1. Please see additional important safety information on next page and accompanying full prescribing information. Submit a separate form for each medication. Please print, type or write legibly in blue or black.
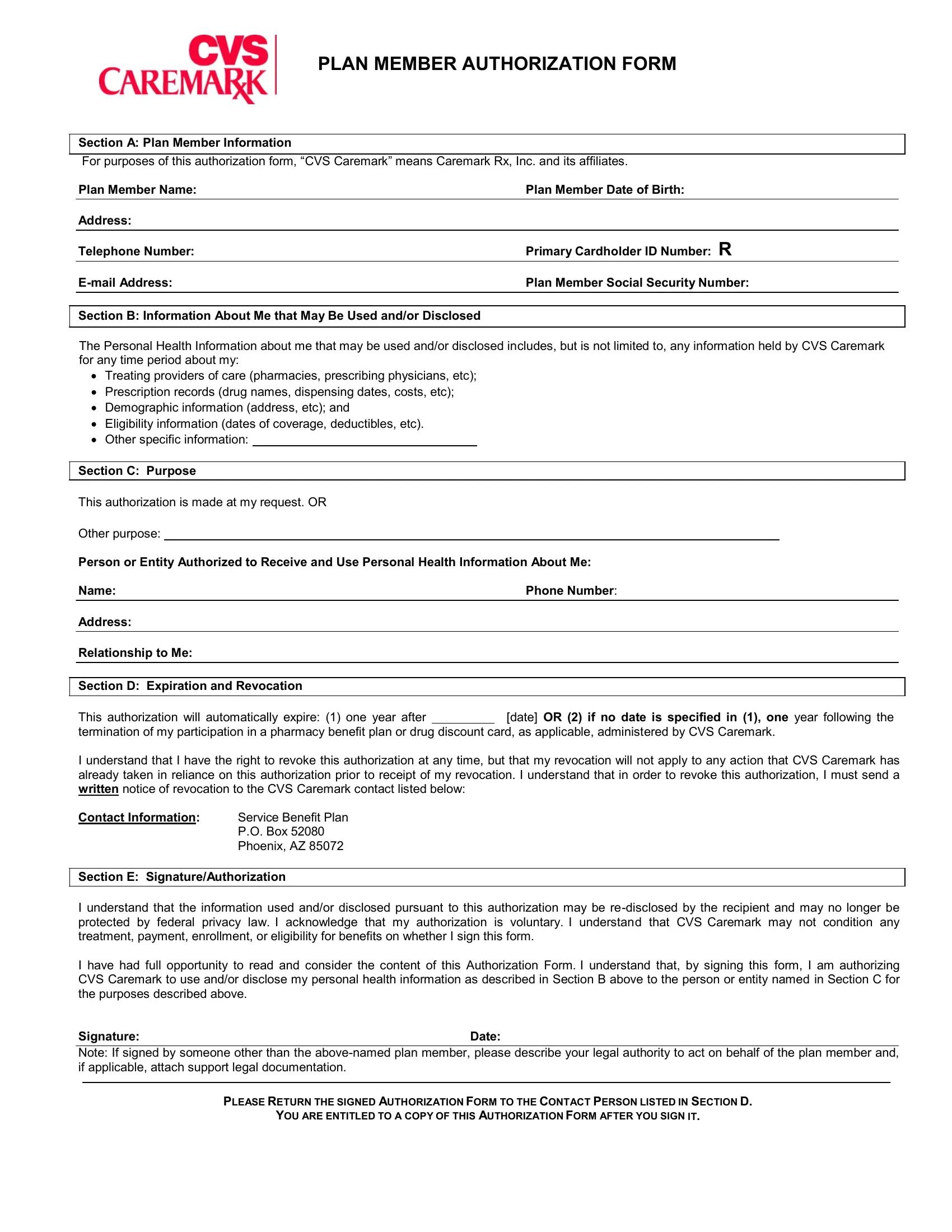
Member Authorization Form ≡ Fill Out Printable PDF Forms Online
Please print, type or write legibly in blue or black. Obtain the appropriate pa form after initiating your patient through one of the following: Please see additional important safety information on next page and accompanying full prescribing information. Dupixent (dupilumab) (preferred) prior authorization form (form effective 1/8/2024) fax to performrx. • dupixent myway ® • covermymeds • insurance provider •.
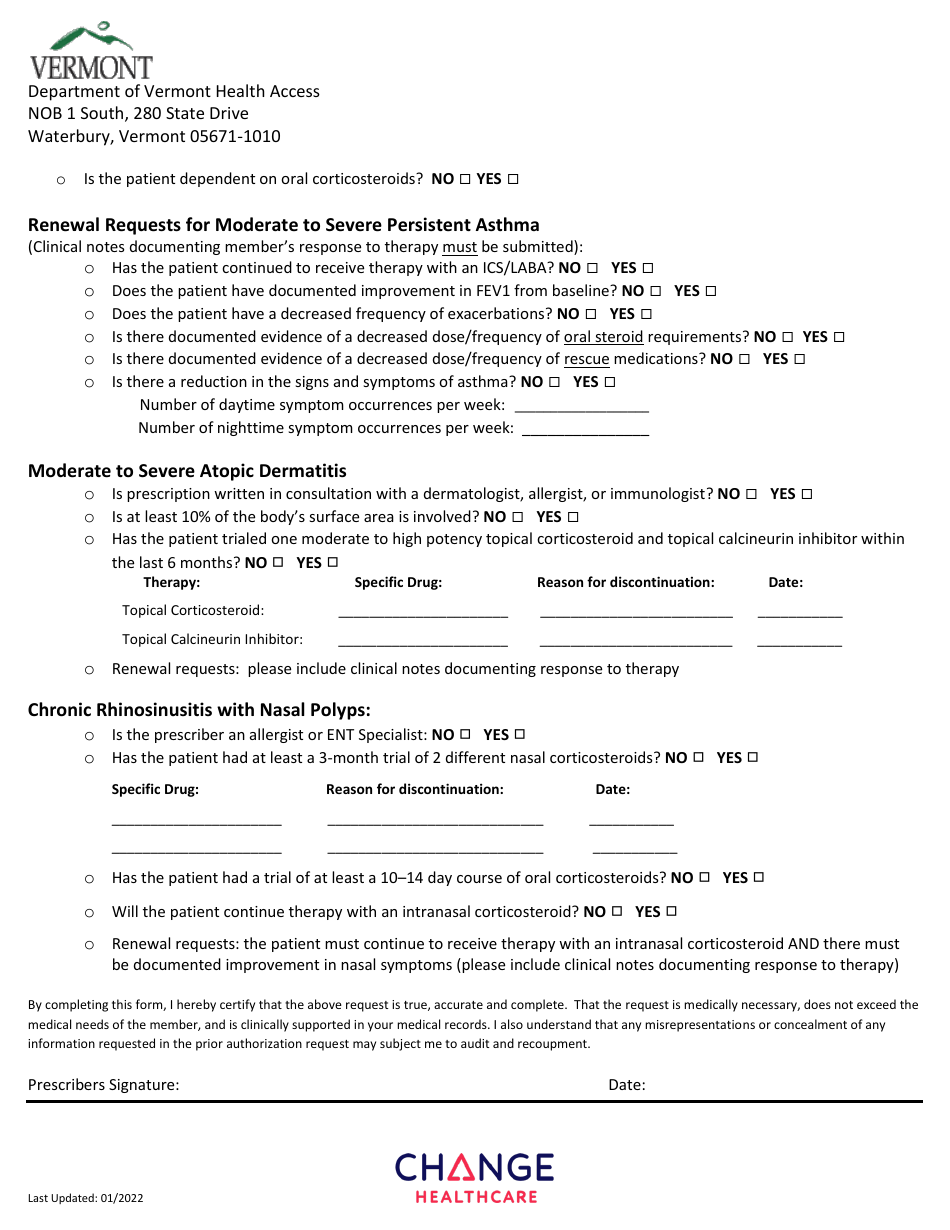
Vermont Dupixent Prior Authorization Request Form Fill Out, Sign
• dupixent myway® • covermymeds • insurance provider •. Please see additional important safety information on next page and accompanying full prescribing information. Dupixent (dupilumab) (preferred) prior authorization form (form effective 1/8/2024) fax to performrx. • dupixent myway ® • covermymeds • insurance provider •. Obtain the appropriate pa form after initiating your patient through one of the following:

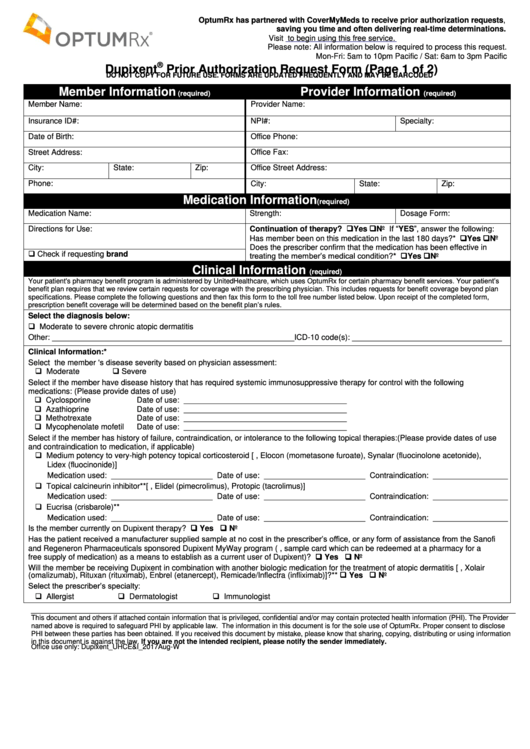
Fillable Online Prior Authorization (PA) Form for Dupixent (dupilumab
Prescribed by one of the following: Instructions for completing this form 1. • dupixent myway® • covermymeds • insurance provider •. Please print, type or write legibly in blue or black. • dupixent myway ® • covermymeds • insurance provider •.
Vermont Dupixent Prior Authorization Request Form Download Printable
Obtain the appropriate pa form after initiating your patient through one of the following: Prescribed by one of the following: Obtain the appropriate pa form after initiating your patient through one of the following: Please see additional important safety information on next page and accompanying full prescribing information. Authorization will be issued for 12 months.

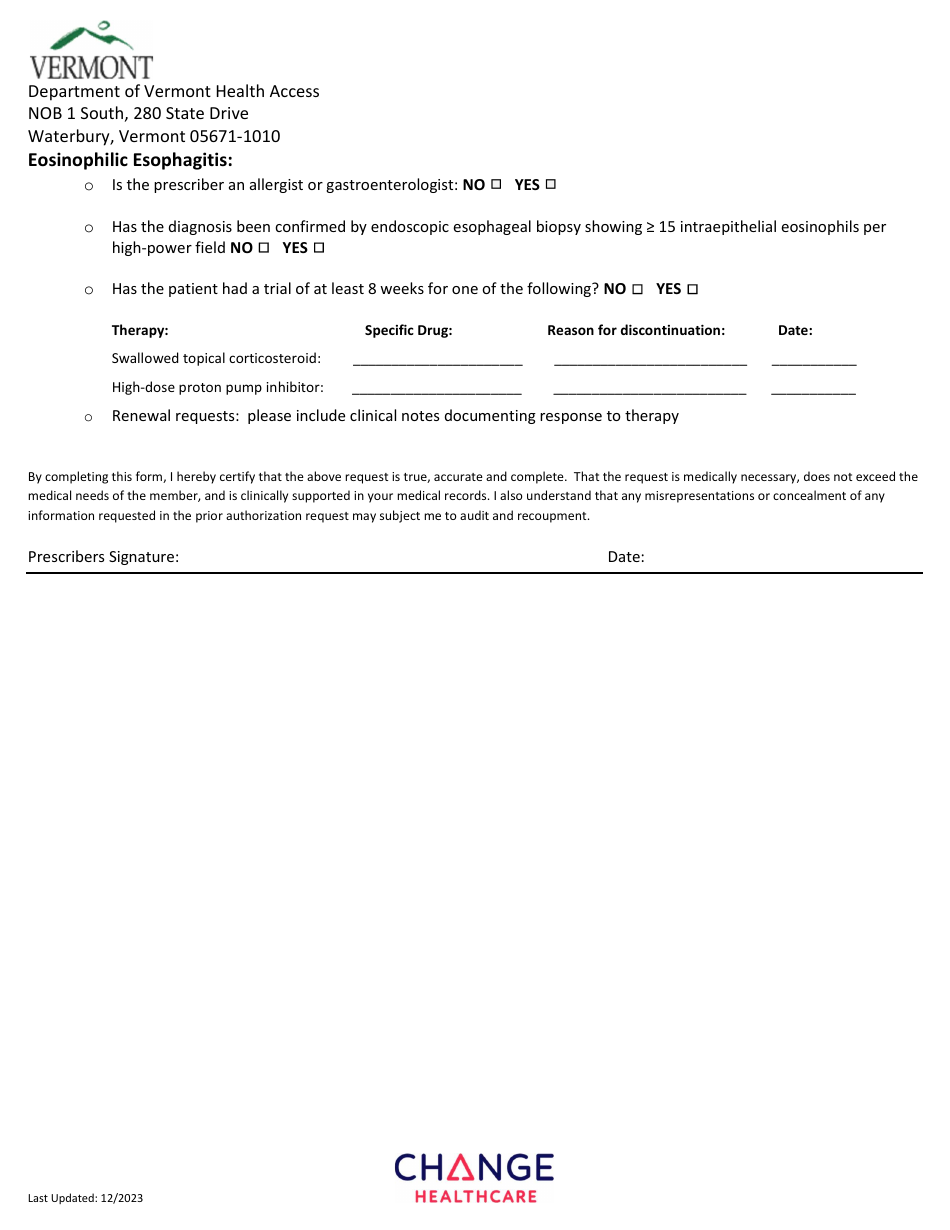
Fillable Online Dupixent Prior Authorization Request Form (Page 1 of 2
Prescribed by one of the following: Obtain the appropriate pa form after initiating your patient through one of the following: Dupixent (dupilumab) (preferred) prior authorization form (form effective 1/8/2024) fax to performrx. Please print, type or write legibly in blue or black. • dupixent myway® • covermymeds • insurance provider •.
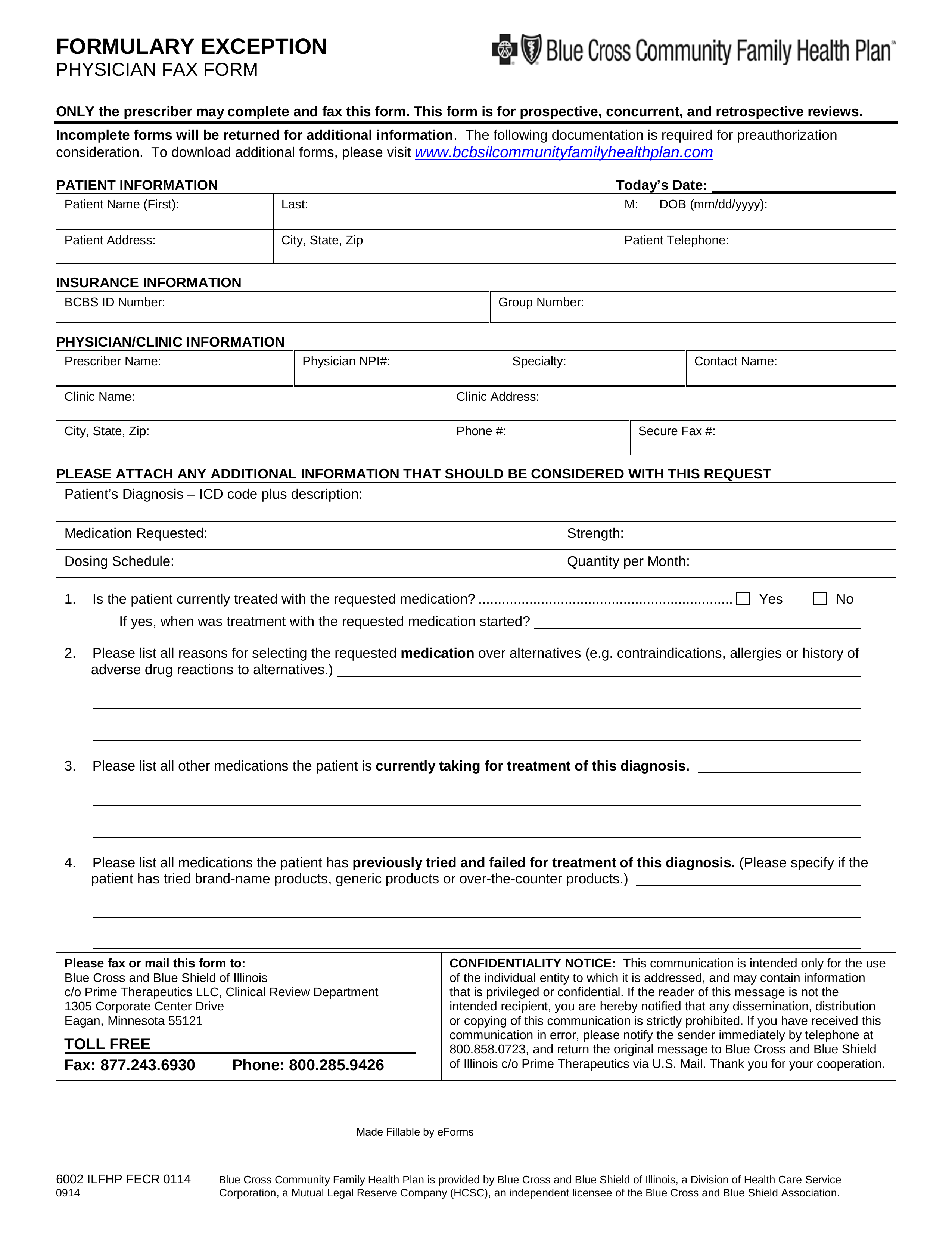
Prime Therapeutics Printable Prior Authorization Form
Prescribed by one of the following: Dupixent (dupilumab) (preferred) prior authorization form (form effective 1/8/2024) fax to performrx. Submit a separate form for each medication. Please see additional important safety information on next page and accompanying full prescribing information. Instructions for completing this form 1.
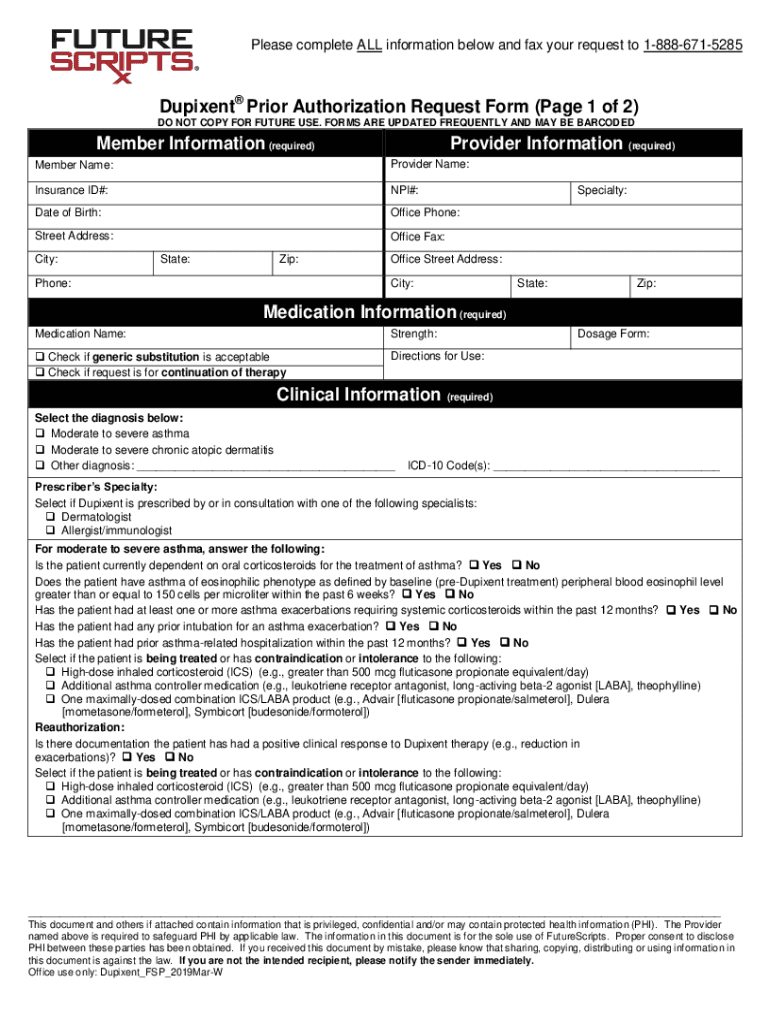
Fillable Online Dupixent Prior Authorization Request Form (Page 1 of 2
Prescribed by one of the following: Instructions for completing this form 1. Obtain the appropriate pa form after initiating your patient through one of the following: • dupixent myway® • covermymeds • insurance provider •. Obtain the appropriate pa form after initiating your patient through one of the following:
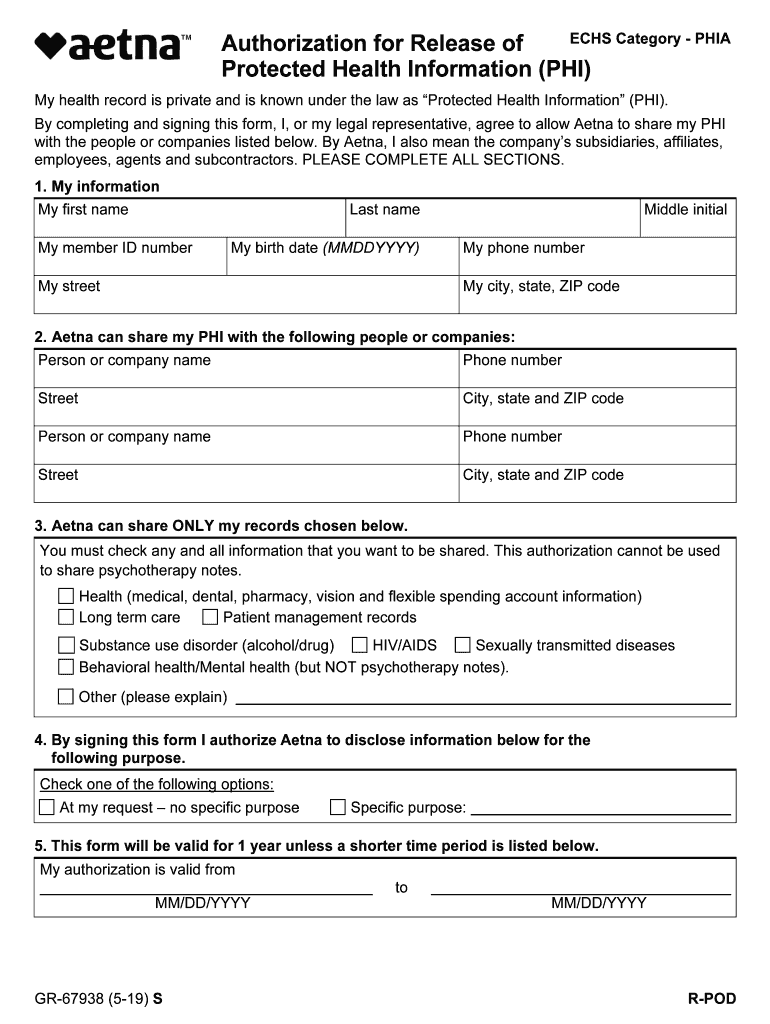
2014 2023 Form Aetna Gr 67353 12 Fill Online Printable Fillable Form
Dupixent (dupilumab) (preferred) prior authorization form (form effective 1/8/2024) fax to performrx. • dupixent myway ® • covermymeds • insurance provider •. Submit a separate form for each medication. Authorization will be issued for 12 months. Prescribed by one of the following:
Dupixent Prior Authorization Request Form printable pdf download
Submit a separate form for each medication. • dupixent myway ® • covermymeds • insurance provider •. Obtain the appropriate pa form after initiating your patient through one of the following: Please print, type or write legibly in blue or black. Reduction in the frequency of exacerbations.
• Dupixent Myway® • Covermymeds • Insurance Provider •.
Instructions for completing this form 1. Reduction in the frequency of exacerbations. Obtain the appropriate pa form after initiating your patient through one of the following: Please print, type or write legibly in blue or black.
Submit A Separate Form For Each Medication.
Obtain the appropriate pa form after initiating your patient through one of the following: • dupixent myway ® • covermymeds • insurance provider •. Please see additional important safety information on next page and accompanying full prescribing information. Authorization will be issued for 12 months.
Prescribed By One Of The Following:
Dupixent (dupilumab) (preferred) prior authorization form (form effective 1/8/2024) fax to performrx.